
SLAP Tears and Biceps Tendon Injuries
Biceps Anatomy

Biceps anatomy - two separate tendons at the shoulder. Short and long heads.
The biceps is often forgotten as a shoulder tendon. It has a muscle belly on the front of the arm that most people know. However, what most people do not realize is that the upper portion of the biceps has two separate tendons. The short-head tendon attaches to bone outside of the shoulder joint. The long-head of the biceps tendon travels into the shoulder joint and attaches to a soft tissue anchor called the labrum of the shoulder. The biceps acts to flex the elbow, rotate the forearm, and to center the humeral head (ball) in the glenoid (socket).
What kind of biceps injuries can happen and what are their symptoms?
This video demonstrates a Biceps tendon tear
Biceps injuries can include strains (muscle stretch) or tendonitis (tendon inflammation) or tears. It is difficult to differentiate between the different diagnoses as they all cause pain. Typically the pain from biceps injuries occurs over the front of the shoulder or deep within the shoulder. The pain is worsened with lifting activities or overhead reaching activities. With certain tears, patients may complain of a "popping" or "clunking" of the shoulder joint.
Where do injuries occur?
Injury to the biceps complex can occur anywhere along its anatomy but at the shoulder joint, the most common location for the biceps to tear happens at either the:
SLAP (superior labrum anterior to posterior) tear. Biceps anchor tear.
long-head biceps tendon as it approaches the joint or along it's course inside the shoulder joint (see video above)
at its insertion on the superior (top part) of the shoulder labrum. This is known as a SLAP tear of the shoulder (see video)
How are SLAP tear and Bicep tendon injuries diagnosed?
These injuries are difficult to assess, but with a combination of thorough history and physical exam along with X-rays and MRI, they can often be detected.
Patient will often report deep and front pain in the shoulder that is difficult to localize. The pain can be associated with a "clunk" or "pop" in the shoulder with overhead or rotational movements.
X-rays are often performed to rule out arthritis or fracture.
MRI is the best test to see a biceps or SLAP tear. Often, the MRI is accompanied by an arthrogram (dye injection into shoulder) to enhance the ability to see even the smallest tears.
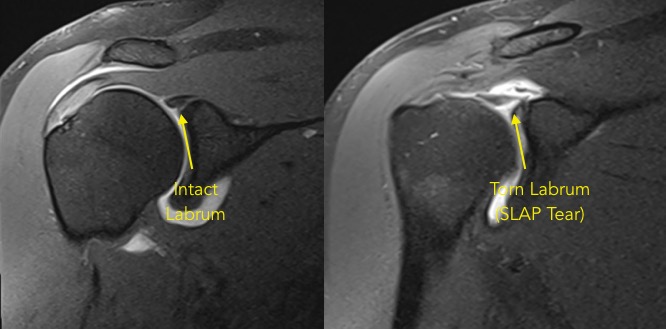
MRI Arthrogram (right) demonstrating a torn biceps anchor or SLAP tear.
What are the treatment options for a biceps tear or biceps anchor tear?
Non-surgical treatment
Many injuries of the biceps tendon and its anchor can be treated conservatively. This treatment path may include modalities such as physical therapy, anti-inflammatory medications, injections, rest, and activity modification.
Surgical treatment is reserved for patients that have continued pain and disability even after a trial of non-surgical treatment
For a biceps tendon tear, very small tears may be debrided or "cleaned up". However, most tears of the tendon are more significant and a surgery is often performed where the tendon is cut within the joint and reattached into the humerus. This is called a biceps tenodesis. This procedure removes the damaged portion of the tendon while still giving the biceps tendon almost normal function and appearance.
For a superior labral tear (SLAP tear), a variety of surgical treatments exist. The choice should be left to the surgeon depending on the degree of the tear, the age of the patient, and the involvement of the biceps tendon. Sometimes, the biceps tenodesis mentioned previously is enough. In other cases, a labral repair can be performed where the torn portion of the labrum is reattached to the edge of the glenoid (socket)...SLAP repair.